Lung cancer 1: Pathology
Author(s): Polyvios Evangelou
Tumour is the Latin word for swelling. It is a very broad term which is sometimes used to refer to an abnormal tissue growth which can be either malignant or benign. In cancer biology, neoplasm is used to describe an abnormal mass of tissue which is undergoing uncoordinated growth and serves no physiological purpose.
Lung tumours (or neoplasms) can be primary, meaning that they arise from lung tissue, or secondary meaning that the lesion comprises of malignant cells that have metastasized to the lung from a distant, primary source.
The vast majority (>90%) of primary lung tumours are malignant.
Lung cancer is the 3rd most common cancer in the UK with 3 in 4 cases being diagnosed at a late stage. It has a poor prognosis with just 10% of patients surviving for 5 years or more after diagnosis and is the leading cause of all cancer-related deaths.
Lung cancer pathogenesis involves accumulation of genetic abnormalities and loss of control of normal cell biological processes (such as cell cycle regulation) in the lung parenchyma. There are recognised environmental factors that increase the risk of developing lung cancer such as cigarette smoking and occupational exposure to carcinogenic substances such as asbestos.
Learning objectives Part 1 of 6
- Provide a macroscopic description of a lung lesion.
- Recall the main types of lung cancer and their classification.
- Recognise the histological features of the main types of lung cancer.
- Understand the pathogenesis of lung cancer.
- Appreciate the principles of targeted drug treatment in lung cancer as an example of personalized medicine.
Macroscopic assessment of lung lesions Part 2 of 6
In this section, we will address the basic principles of macroscopic assessment of tissue specimens using lung lesions in pneumonectomy specimen as examples.
In the following image, we see a cream coloured lesion, centrally located around the hilar area. The lesion has an irregular border and its colour is markedly paler compared to the surrounding brown coloured, healthy lung.

The following image shows a peripheral, cream coloured lesion with a necrotic core and irregular border. Interlobular satellite lesions are present (left side of the image) which might represent metastatic lung disease.

This last image shows a cream, peripheral lung lesion, with a purple core, irregular border. Arrow indicates pleural puckering.
Now you may use the following image to complete the macroscopic description that follows.

Main types of lung cancer Part 3 of 6
There are many types of lung cancers but for the purposes of this module we will focus on the 3 most prevalent:
- Small cell carcinoma
- Lung adenocarcinoma
- Squamous cell carcinoma
These types are classified into two categories:
- Small Cell Lung Cancer (SCLC)
- Non-Small Cell Lung Cancer (NCSLC)
- Lung adenocarcinoma
- Squamous cell carcinoma
SUMMARY TABLE

Microscopic features lung cancer Part 4 of 6
Lung adenocarcinoma
- Most common type of lung cancer.
- Around 2/3 are peripherally located in the lung.
- Classified into the following types:
- Lung Adenocarcinoma in situ: refers to non-invasive adenocarcinoma
- Minimally Invasive Adenocarcinoma: the lesion macroscopically measures no more than 3 cm and microscopically involves no more than 5 mm stromal invasion.
- Invasive adenocarcinoma: refers to any adenocarcinoma tumour that surpasses the above measurements and invades the stroma more than 5 mm.
Invasive adenocarcinomas can show the following histological patterns:
- Acinar
- Lepidic
- Solid
- Papillary
- Micropapillary

The image above is an H&E stained lung tissue specimen with evidence of glandular growth pattern (*).
Squamous cell carcinoma
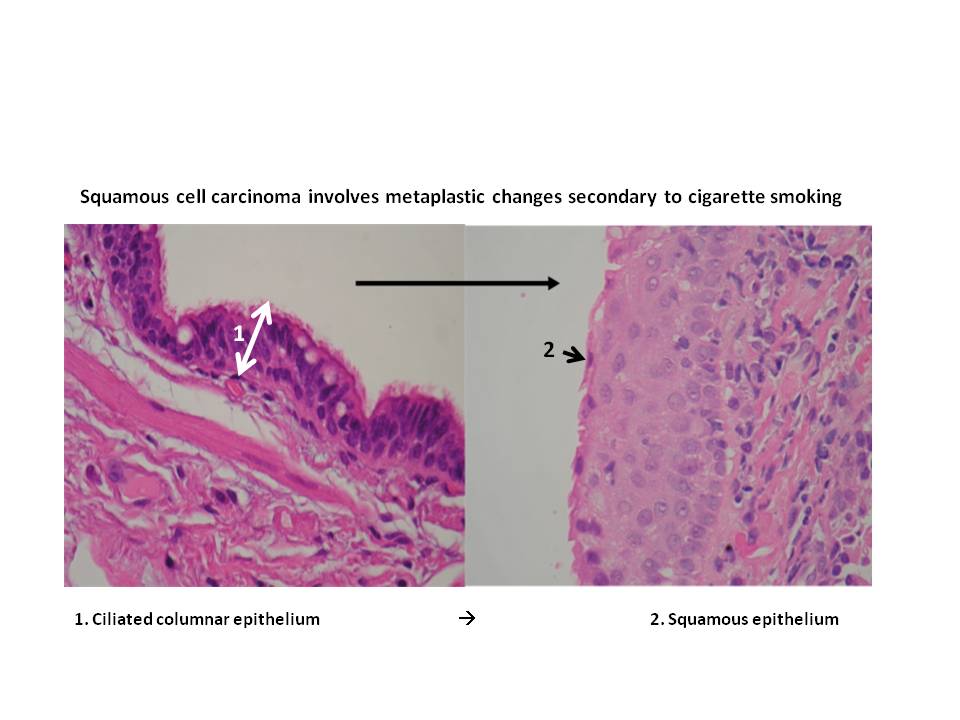
- Type of lung cancer most closely associated with cigarette smoking
- Arises from metaplasia of the ciliated columnar bronchial epithelium to squamous.
- Since squamous metaplasia commonly occurs in the bronchi, squamous carcinoma is commonly found centrally near or within the lung hilum.
- Squamous cell carcinoma often exemplifies invasive growth within the bronchus as well as the surrounding soft tissue, lymph nodes and lung parenchyma.
- Endobronchial and peribronchial growth can lead to bronchopneumonia and atelectasis.

The above image is an H&E histological section of a lung lesion showing tumour cells with squamous differentiation.
Small cell lung carcinoma
- Most aggressive type of lung cancer
- Highly malignant, metastasizes early
- Advanced stage at diagnosis with poor prognosis
- Microscopically cells appear as if they have crashed into one another, exemplifying a ‘nuclear moulding’.
- Neuroendocrine in origin thus sometimes can ectopically secrete hormones such as ACTH and ADH leading to paraneoplastic syndromes.

Small cell undifferentiated carcinoma
The following question aims to summarize the main points discussed above.
Lung cancer pathogenesis Part 5 of 6
‘Pathogenesis’ and ‘aetiology’ are two terms that are commonly used interchangeably. Nevertheless, each refers to a slightly different concept. Aetiology refers to the causative agents of a disease (e.g. cigarette smoking) whereas pathogenesis is the mechanism or sequence of events (e.g. hyperplasia, metaplasia, dysplasia) through which the underlying aetiological factors give rise to a disease (e.g. lung cancer).
Development of lung cancer is a multi-step process of physiological insults (aetiological factors) such as radiation exposure, inhalation of noxious chemicals (e.g. cigarette smoke, asbestos), converging to the accumulation of genetic abnormalities causing defects in regulatory cell processes and normal homeostasis such as:
- cell cycle signaling
- regulation of apoptosis
- angiogenesis pathways
Some pathologies (e.g. Li Fraumeni syndrome, pulmonary fibrosis. Human Papilloma Virus infection) are considered to predispose patients to the development of lung cancer because of increased risk for accumulation of genetic abnormalities.
Specific types of lung cancer are affected by specific types of mutations. For example, approximately a quarter of lung adenocarcinoma express a mutated EGFR gene leading to prolonged cell survival and neoplasia.
The following table summarizes the main aetiological factors that can be implicated in lung cancer and an overview of the general principle leading to lung cancer. Detailed analysis of lung cancer pathogenesis is beyond the scope of this tutorial.

Principles of personalized medicine Part 6 of 6
Personalised medicine involves targeted drug treatment dependent on the specific gene mutation(s) implicated in an individual patient’s disease.
In lung cancer, there is a variety of gene mutations that might be implicated such as EGFR, ALK, PD-1, KRAS, ROS-1.
Presence of a mutation in any of these genes has therapeutic significance as the patient can receive drug treatment targeting the affected gene (targeted drug treatment).
- e.g. EGFR inhibitors can be used for a patient with lung adenocarcinoma that is positive for EGFR mutation.
- Nevertheless, not all lung adenocarcinomas have mutations in genes for which a drug inhibitor has been developed. Those tumours that test negative for targetable gene mutations are not candidates for targeted drug treatment.
Targeted drug treatment is therefore decided on a case by case basis depending on the specific genetic profile of each patient’s lung cancer. Thus the term ‘personalised medicine’