Neoplasia – definition, nomenclature and spread
Author(s): Mark Arends
Learning objectives
By the end of this CAL you should be able to:
- Define the term neoplasia and explain how tumours are named
- Describe how a neoplasm grows and spreads and state the sites to which the common ones tend to go
Definitions - Neoplasm Part 1 of 11
The term neoplasm refers to the tumour mass itself. The process that occurs to produce a neoplasm is called neoplasia.
Willis defined a neoplasm as “an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the surrounding normal tissues, and persists in the same excessive manner after cessation of the stimuli which evoked the change”. (For example, once a lung cancer has developed, it doesn’t go away if the individual stops smoking.).
Neoplasms have an increase in cell numbers that must be distinguished from the reversible increase in cell number (hyperplasia such as in enlarged prostates of older men) or cell size (hypertrophy such as in the enlarged uterus of pregnancy) that may also be seen in larger organs.
Essential features of neoplasia or tumour growth include:
- Tumours are composed of living cells, which differ from the cells of the normal organ from which the tumour is derived in that the cell division, cell death and cell differentiation controls operating in that tissue or organ have been deregulated or lost
- The control of cell division, death and differentiation may have been lost to the extent that the tumour:
- (a) loses partially or totally specialised functions (cell appearance changes)
- (b) acquires new functions such as invasion – the capacity to infiltrate the surrounding tissues and organs and metastasis – the ability to spread to and proliferate in distant parts of the body after tumour cells have been transported by lymph or blood or along body spaces
Definitions - benign and malignant Part 2 of 11
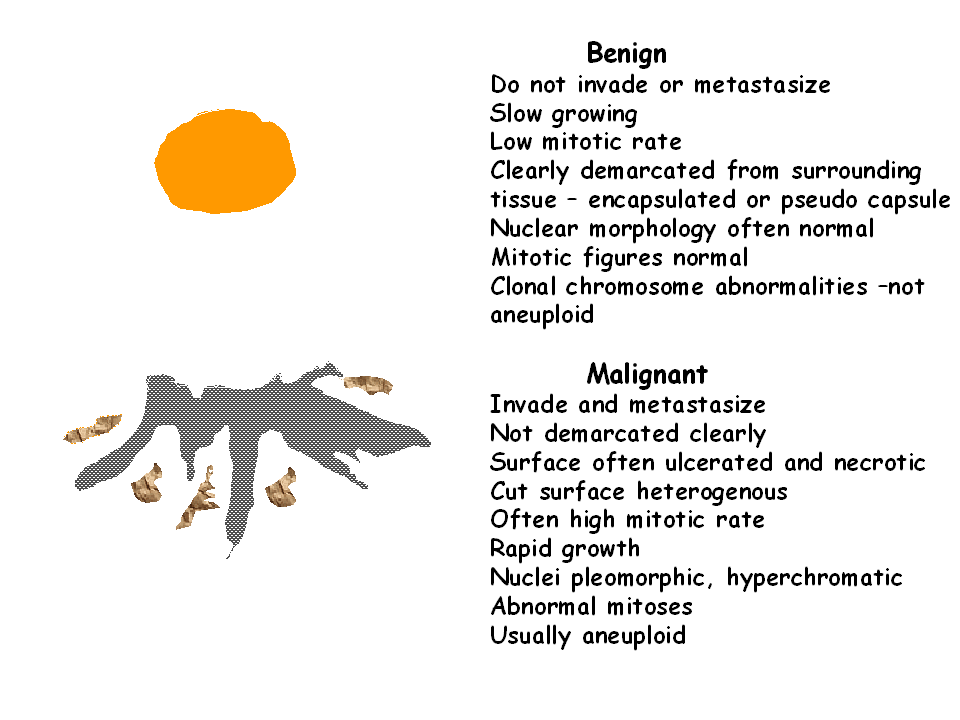
Neoplasms are divided into benign and malignant.
Benign neoplasms do not invade or metastasise (spread), whereas malignant neoplasms show evidence of invasion (or infiltration) into adjacent tissues, often in a destructive way and many will undergo metastasis (spread to other sites in the body to form secondary tumours – the original is often called a primary tumour).
Benign tumours
Benign tumours are those which proliferate and divide but do not invade the surrounding tissues, nor metastasize. Such benign neoplasms or tumours and the use of the term benign implies that their growth is not life-threatening, and their clinical course is predictable. They may cause problems due to pressure, obstruction or excessive hormone production.
Malignant neoplasms
Neoplasms which invade and/or metastasise are malignant neoplasms (often called cancers in ordinary language). Their clinical course is progressive; unless adequate therapy is available the patient will eventually die as a result of the disease.
Cancers show destructive invasive growth behaviour and can produce signs and symptoms such as:
- Blood loss – ulceration and haemorrhage
- Pressure and destruction of adjacent tissue
- Obstruction or constriction of flow in vital organs
- Metabolic effects: general – cachexia (severe weight loss including a reduction in muscle mass); and specific – production/secretion of tumour-specific products/hormones
Question Part 3 of 11
Nomenclature - types of neoplasm Part 4 of 11
The name of the tumour usually refers to the cellular origin and behaviour of the neoplasm.
Some common neoplasms are named as follows:
- Benign neoplasm of glandular tissue is an adenoma; malignant is an adenocarcinoma
- Benign neoplasm of squamous epithelium is a papilloma; malignant is a squamous cell carcinoma
- Benign neoplasm of fat is a lipoma; malignant is a liposarcoma
- Benign neoplasm of smooth muscle is a leiomyoma; malignant is a leiomyosarcoma


Benign tumours of connective tissue
- Adipocytes – lipoma
- Fibrocytes – fibroma
- Chondrocytes – chondroma
- Smooth muscle – leiomyoma
- Striated muscle – rhabdomyoma
- Bone – osteoma
Malignant tumours arising from connective tissues
Malignant tumours arising from connective tissues are called SARCOMAS and further classified by the cell of origin:
- Fibrocytes – fibrosarcoma
- Osteoblasts – osteosarcoma
- Chondrocytes – chondrosarcoma
- Smooth muscle – leiomyosarcoma
- Striated muscle – rhabdomyosarcoma
Neoplasms of germ cells
Germ cells are cells in testis or ovary that can form any of the tissues derived from the three germ layers of the embryo in normal circumstances – ectoderm, mesoderm or endoderm.
Benign tumours of germ cells are called teratomas. Malignant tumours arising from germ cells are teratocarcinomas (or malignant teratomas).
Haemopoietic system tumours
Haemopoietic system tumours are a special case as they derive from the haematopoietic stem cells in the bone marrow that have acquired various mutations and now generate large numbers of neoplastic cells that flood out of the marrow and into the blood) and the suffix – aemia – relating to blood – is applied to them:
Leukaemia – cancer of white blood cells in the blood
The classification of leukaemias is based on:
- their clinical course – acute or chronic
- the cell lineage – myeloid or lymphoid
The 4 major types are acute myeloid leukaemia, chronic myeloid leukaemia, acute lymphoid leukaemia, chronic lymphoid leukaemia.
Myeloid refers to the granulocytic (e.g. neutrophils) or monocytic / macrophage and related lineages; whereas lymphoid refers to the lymphocytic lineage – both describe the lineage/type of neoplastic cells.
Tumour Nomenclature Exceptions
Sometimes names persist for historical reasons, such as melanoma of the skin, or seminoma of the testis, or lymphoma in the lymph nodes, all of which are malignant and life-threatening (despite ending in –oma).
Nomenclature - tumour grade Part 5 of 11
Malignant neoplasms are further described by the histopathologist on the degree to which the histological appearance and architecture of the tumour resembles that of the normal organ or tissue from which it was derived.
This is referred to as the differentiation of a tumour (well, moderately, poorly differentiated) or grade (G1, G2, G3).
This information is of use in determining treatment and prognosis. Poorly differentiated (high (G3) grade) tumours usually demonstrate a more aggressive behaviour.
Nomenclature - tumour stroma Part 6 of 11
A tumour consists of the neoplastic cells and a vascularised connective tissue support of stroma. This is particularly marked in epithelial tumours.
The stroma is not neoplastic but is a host response to tumour growth. Cancer-associated fibroblasts (CAF) secrete desmoplastic stroma.
Neovascularisation (new blood vessel growth through angiogenesis) of tumours is essential if they are to grow.
The extent and composition of the stroma depend upon the molecular signals from the tumour cells.
Question Part 7 of 11
Nomenclature - tumour spread Part 8 of 11
Invasiveness is the distinguishing characteristic of malignancy. This confers on malignant cells the ability not only to infiltrate local tissues but to invade:
- lymphatics and reach lymph nodes
- blood vessels and spread to distant sites (liver, lung, bone and brain are the 4 most common sites for metastasis of carcinomas)
- tissue spaces (transcoelomic spread – such as ovarian cancer spreading through the peritoneal cavity to form multiple small nodules studded over the intestines, liver and other abdominal organs) and hence produce remote metastasis

Nomenclature - tumour stage Part 9 of 11
Tumour stage is a measure of how advanced the tumour has become in primary growth and secondary (metastatic) spread.
It is used to guide postoperative treatment of cancer patients (after surgical removal of the primary tumour mass).
A commonly used system is the TNM system where:
- T (e.g. T1, T2, T3, T4) represents increasing primary tumour size or local invasion into adjacent tissues
- N represents the lack of spread to nodes (N0) or spread to one or a few nodes (N1) or many nodes (N2)
- M represents evidence of lack of metastasis (M0) or metastatic spread to distant organs such as the liver or lungs (M1)

Question Part 10 of 11
Summary Part 11 of 11
Increased cell proliferation in response to increased demand for function – hyperplasia – is tightly and normally controlled.
Neoplasia is uncontrolled proliferation and manifests as neoplasms (tumours):
- Benign neoplasms proliferate but do not invade adjacent tissue
- Malignant neoplasms proliferate, invade adjacent tissues and/or metastasise (separate from parent tumour and grow in distant parts)
Malignant tumours are cancers. Cancers metastasise via:
- blood (haematogenous spread)
- lymph channels (lymphatic spread – often to nodes)
- along body spaces (transcoelomic spread, such as peritoneal or pleural or pericardial cavities), or by direct invasion to adjacent organs (such as prostate cancer invading into the rectum)