Mental State Examination 2 – Speech and Thought
Author(s): Farah Rozali
Learning outcomes
By the end of this CAL you will be able to:
- Describe the general purpose and component parts of the Mental State Examination (MSE), specifically patients’ speech and thought.
- Evaluate patients’ speech and thought in their mental state and use appropriate terminology to describe abnormalities.
Acknowledgments:
Thank you to Neelom Sharma, Alexandra Pittock, Meroe Grove, Maia Forrester and Mercedes Smith for their major contributions to the content of this module.
Introduction Part 1 of 11

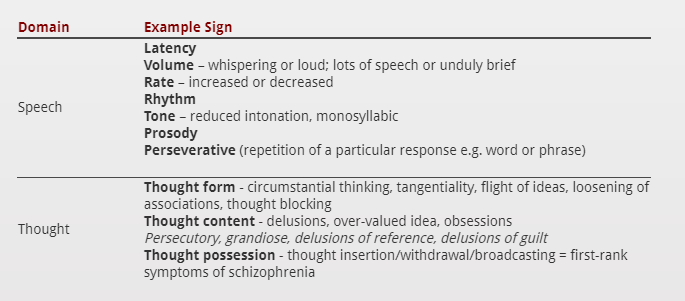
Speech and Thought Part 2 of 11
Speech Part 3 of 11
Thought Part 4 of 11
Thought Form Part 5 of 11
Thought form deals with the ‘mechanics’ of the patient’s thoughts i.e. how the patient is thinking. This is of diagnostic use as in many psychiatric disorders, thinking ‘slips’ to a less sophisticated level as a consequence of the illness.
This results in disorders of thought form, where the ability to express ideas cogently and coherently is compromised or lost completely. The stream of goal-directed thought is disrupted by irrelevancies to the extent that the goal gets lost.
The first thing to note, therefore, is how easy is it for you to follow what the person is saying…
Do you have a sense of where they are going with their thoughts?
- Do they go off on a lot of tangents?
- Do they seem to be including too much information?
- Do they eventually get to the ‘goal’ or not?
- Do their thoughts seem to jump from one ‘connection’ to another really quickly?
- Are these break-points logical or is it hard to see the connections?


Thought Content Part 6 of 11
Delusions Part 7 of 11
Overvalued Ideas Part 8 of 11
An overvalued idea is a plausible belief that a patient becomes pre-occupied with to an unreasonable extent. The key feature is that the pursuit of this idea cause considerable distress to the patient or those living around them.
They are distinguished from delusions by the lack of gross abnormality in reasoning; these patients can often give fairly logical reasons for their beliefs.
They differ from obsessions in that they are not seen as recurrent intrusions.
Thought Possession Part 9 of 11
Questions Part 10 of 11
Summary Part 11 of 11