Chronic inflammation
Author(s): Tim Kendall
Learning outcomes
By the end of this CAL you will be able to:
- Understand the context of chronic inflammation.
- Describe macrophage activation.
- Define the role of the macrophage as a key orchestrator of chronic inflammation.
Introduction Part 1 of 7
Chronic inflammation is one of the possible outcomes of acute inflammation.

Causes of chronic inflammation
Chronic inflammation can occur due to:
- Persistent infections (e.g. tubercle bacillus)
- Persistent toxic agents (silica)
- Auto-immunity
Cells of chronic inflammation
Numerous inflammatory cells can be involved in chronic inflammation. These include:
- Macrophages
- Endothelial cells
- Fibroblasts
- Lymphocytes
- Eosinophils
Macrophages in chronic inflammation Part 2 of 7
Tissue macrophages are derived from the bone marrow in an immature form – monocyte.
They are slower to accumulate at sites of inflammation.
They are:
- Effector cell with a phagocytic role
- Mediator cells, the “conductor of the inflammatory orchestra”

Activation of macrophages
Macrophages are activated by other components of the inflammatory milieu:
- Endotoxin
- Interferon-γ from T cells
- Natural Killer (NK) cells
After activation, macrophages increase their:
- Size
- Metabolism
- Levels of lysosomal enzymes
- Phagocytic activity
- Ability to kill phagocytosed micro-organisms
However, they can also cause bystander tissue damage.
Macrophages as effector cells
Macrophages are capable of exerting their own direct influence by acting as effector cells. They can:
- Phagocytose and kill micro-organisms
- Phagocytose cell debris
- Phagocytose foreign material
This prepares the local environment for granulation tissue formation (angiogenesis and extracellular matrix deposition).
Macrophages as mediators

Activated macrophages produce a panoply of soluble mediators including:
- Platelet-derived growth factor
- Fibroblast growth factor
- Transforming growth factor β
All of these stimulate fibroblasts in different ways. PDGF can promote angiogenesis. This combination leads to granulation tissue formation.
Role of lymphocytes and eosinophils in chronic inflammation Part 3 of 7
Lymphocytes in chronic inflammation
- Add specificity to macrophage response
- Give rise to plasma cells secreting antibodies
- Can be cytotoxic
Eosinophils (EΦ) in chronic inflammation
- Attracted by substances released by macrophages
- Major basic protein kills helminthic parasites (schistosomiasis etc.)
Plasma cells in chronic inflammation
Plasma cells that produce antibody. They are generated from B lymphocytes. They have:
- Nucleus at one end of the cell (a)
- Chromatin in coarse blobs beneath the nuclear membrane (b)
- Basophilic cytoplasm (c)

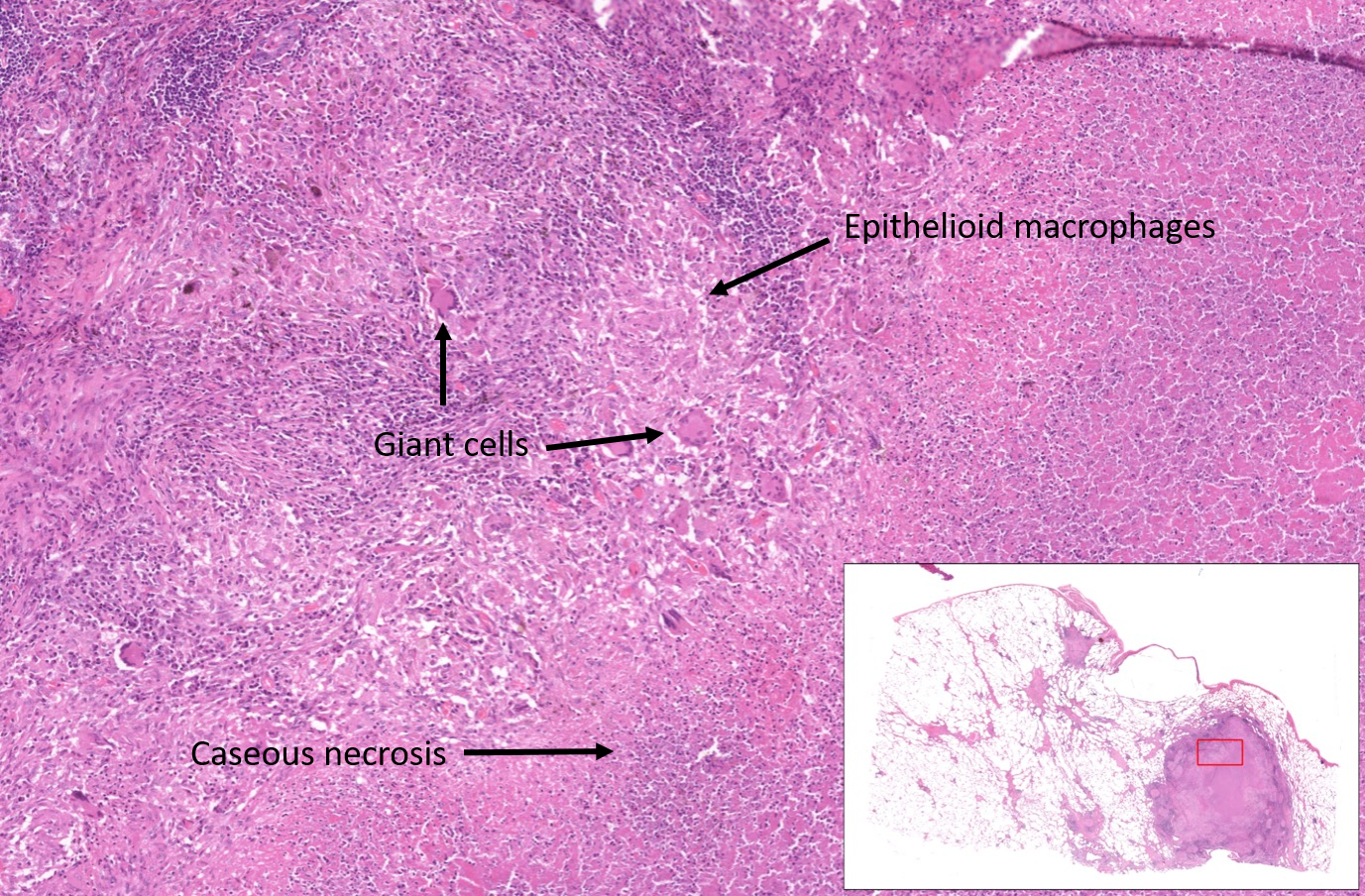
Granulomatous inflammation Part 4 of 7

Granulomas form by the accumulation of macrophages with ‘harder, denser’ cytoplasm (epithelioid cells) and multinucleated giant cells. They are associated with TB, sarcoidosis, leprosy etc.. They can be seen with foreign bodies and in autoimmune disease. Caseous necrosis can be found in the centre of large granulomas in mycobacterial infection.
Systemic response to injury Part 5 of 7
Systemic inflammatory mediators induce a range of systemic effects:
- Fever
- Acute phase reaction proteins production (CRP, fibrinogen, serum amyloid A)
- Metabolic changes, the breakdown of muscle protein, changes in glucose metabolism – prepares for starvation
These changes modify the environment in which inflammatory response takes place. Macrophage-derived IL-1 is a critical mediator.
Summary Part 6 of 7
Inflammation is an adaptive response that:
- Removes injurious stimulus
- Initiates healing
- Is usually beneficial